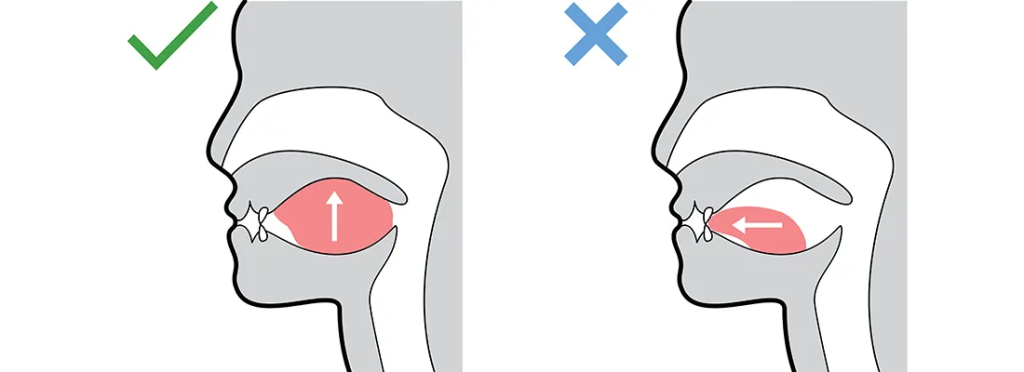
NASAL BREATHING VS MOUTH BREATHING




Nasal breathing is a pillar of health generally and without it, disease progression is a slow grind onwards.

The obvious signs of which will be seen with:
- Dry mouth in the patient,
- Chapped lips from the air going across them all the time,
- Bad breath
- Inflamed gums
- Gingivitis
- Increase dental decay and plaque due acidification of the mouth
- Decline in the saliva production

Open mouth breathing for any reason is associated with a phenomenon called cranial developmental drift, both causally in infants and children, and as a result of cranial maldevelopment.
As the children’s face slowly deviate away from normal growth pattern, this leads to an adult with structural postural change including a long face, narrow through the jaw and maxilla, this is also called an adenoid face.
Maldevelopment patterns include:
- More prominent protruding teeth
- Incapacity to keep the lips sealed
- Retrusion of the mandible
- Slackening off the jaw and jaw muscles
- Teeth will then tend to become crowded and crooked
The narrow palette with the high arch is an airway risk factor which is associated with disturbed sleep and breathing (OSA) leading to consequences in adulthood.

